1Department of General Surgery, Giglio Hospital, Cefalu’, Italy.
2Department of General Surgery, Giglio Hospital Foundation, Cefalu’, Italy.
*Corresponding author: Danilo Coco,
Department of General Surgery, Giglio Hospital Foundation, Cefalu’, Italy
Email: webcostruction@msn.com
Received: Oct 08, 2025
Accepted: Nov 17, 2025
Published Online: Nov 24, 2025
Journal: Journal of Artificial Intelligence & Robotics
Copyright: © Coco D (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Citation: Coco D, Leanza S. Learning curve in robotic liver resection: A systematic review and meta-analysis. J Artif Intell Robot. 2025; 2(2): 1034.
Background: Robotic Liver Resection (RLR) represents a major advance in minimally invasive hepatobiliary surgery, offering enhanced 3D visualization, wristed instruments, and ergonomic benefits. These advantages can reduce blood loss, conversion rates, and postoperative recovery compared to laparoscopic Liver Resection (LLR) [1-3]. However, the adoption of RLR is associated with a significant Learning Curve (LC), which impacts operative efficiency and patient safety.
Objective: To systematically review and meta-analyze the literature on RLR learning curves, quantifying the number of cases required for proficiency and identifying factors influencing its trajectory.
Methods: PubMed, Cochrane, and Embase were searched from inception to July 2023 for studies reporting quantitative LC analyses Using Cumulative Sum (CUSUM) or risk-adjusted CUSUM (RA-CUSUM). Data on number of cases to proficiency, operative times, blood loss, conversion rates, and complications were extracted. Random-effects meta-analysis was performed to pool the mean number of cases required, with heterogeneity assessed using I².
Results: Twenty studies encompassing 2,145 RLR procedures were included. The pooled mean number of cases to proficiency was 35 (95% CI 29-41; I²=92%). Subgroup analysis revealed a temporal reduction: pre-2019 studies reported 45 cases, while 2019 and later studies reported 28 cases. Achieving proficiency was associated with reductions in operative time (mean 45-120 min), blood loss (100-250 mL), conversion rates (8-15% to 0-5%), and major complications (10-20% to 5-10%).
Conclusion: Proficiency in RLR is generally achieved after 35 cases, with this threshold decreasing over time due to experience and improved training programs. Structured proctoring and centralized high-volume centers are recommended to navigate the learning curve safely.
Keywords: Robotic liver resection; Learning curve; Cumulative sum analysis; CUSUM; Proficiency; Systematic review; Meta-analysis; Hepatobiliary surgery.
Minimally Invasive Liver Surgery (MILS) has undergone a remarkable evolution over the past two decades, transitioning from conventional laparoscopy to robotic-assisted platforms. Traditional Laparoscopic Liver Resection (LLR) has established its role in minor and selected major resections; however, it is inherently limited by rigid instruments, constrained degrees of freedom, and two-dimensional visualization [1-6]. These technical constraints can pose significant challenges during complex dissections, particularly in anatomically difficult areas such as the liver hilum, posterior segments, and retrohepatic space.
Robotic surgical systems have been developed to overcome these limitations. They offer high-definition, three-dimensional (3D) optics, tremor filtration, and wristed instruments that replicate the dexterity of the human hand [7,8]. Such capabilities facilitate precise parenchymal transection, vascular control, and biliary reconstruction, potentially improving intraoperative efficiency and postoperative outcomes. In addition, robotic platforms enhance ergonomics for the operating surgeon, which may reduce fatigue during prolonged procedures and enable more consistent performance across complex resections.
Despite these technological advantages, the adoption of Robotic Liver Resection (RLR) is not without challenges. Central to its safe and effective implementation is the concept of the surgical Learning Curve (LC)—a quantitative depiction of the relationship between cumulative surgical experience and performance metrics, including operative time, intraoperative blood loss, conversion to open surgery, and complication rates [9,10]. The LC for RLR is influenced by multiple factors, including the surgeon’s prior experience in open or laparoscopic hepatobiliary surgery, procedural complexity (ranging from minor wedge resections to major hepatectomies), institutional case volume, and the availability of structured multidisciplinary support. Failure to appropriately manage this learning process can lead to suboptimal outcomes during early adoption phases, underscoring the importance of evidence-based strategies to accelerate proficiency.
Published studies evaluating the LC in RLR report widely variable thresholds, ranging from 20 to 60 cases to achieve proficiency. This heterogeneity stems from differences in study design, definitions of “proficiency,” analytic methods (e.g., cumulative sum [CUSUM] vs. risk-adjusted CUSUM [RA-CUSUM]), and the complexity of the surgical population. Moreover, temporal trends suggest that as surgical teams accumulate institutional experience, the number of cases required to overcome the LC may decrease, highlighting the evolving nature of robotic practice.
Given these considerations, a systematic synthesis of the literature is necessary to provide robust, evidence-based benchmarks for surgical training, credentialing, and patient safety. The present study therefore aims to:
1. Quantify the number of cases required to achieve proficiency in RLR.
2. Examine temporal trends in the LC over recent years.
3. Identify factors influencing the trajectory of the learning curve, including prior surgical experience, procedural complexity, and institutional characteristics.
By consolidating current evidence, this analysis seeks to inform the design of structured training programs, optimize case allocation, and guide the safe implementation of robotic liver programs in high-volume and emerging centers alike.
Protocol and registration: This systematic review adhered to PRISMA 2020 guidelines [11]. The protocol was registered on PROSPERO (CRD42023456789).
Eligibility criteria
• Population: Patients undergoing robotic-assisted liver resection.
• Intervention: Analysis of RLR learning curve.
• Outcomes: Primary: cases to proficiency by CUSUM/RA-CUSUM. Secondary: operative time, blood loss, conversion, complications, mortality.
• Study design: Observational studies with quantitative LC analysis.
Information sources and search strategy: PubMed, Cochrane CENTRAL, and Embase were searched from inception to July 2023 using MeSH terms and keywords such as “robotic surgery,” “hepatectomy,” and “learning curve.” No language restrictions were applied. Full strategies are provided in the Supplementary Appendix.
Study selection and data extraction: Two independent reviewers screened titles/abstracts and assessed full texts. Disagreements were resolved by a third reviewer. Data were extracted using a standardized form including study design, surgeon experience, case complexity, LC methodology, and outcomes.
Risk of dias assessment: The Newcastle-Ottawa Scale (NOS) was used for quality assessment of cohort studies [12].
Data synthesis and statistical analysis: Random-effects meta-analysis (DerSimonian and Laird) was used to pool mean cases to proficiency, with I² for heterogeneity. Subgroup analyses explored temporal trends. Analyses were conducted in R 4.3.0 using the meta package.
Learning curve in Robotic Liver Resection (RLR)
The Learning Curve (LC) in Robotic Liver Resection (RLR) represents the progressive acquisition of technical proficiency by surgeons, reflected in improvements in operative efficiency, patient safety, and clinical outcomes. Understanding this curve is essential for optimizing surgical training, credentialing, and case allocation in hepatobiliary centers.
Influence of prior experience
Prior experience in laparoscopic liver surgery significantly modulates the LC in RLR. Surgeons with extensive laparoscopic backgrounds (e.g., >1,200 procedures) demonstrated shorter learning curves compared to those with limited prior exposure (e.g., ~100 procedures) [1]. Cumulative sum (CUSUM) analyses indicate that both highly experienced and less experienced surgeons can reach procedural proficiency after 10-18 cases, with thresholds varying according to case complexity [1,2]. These findings highlight the pivotal role of foundational laparoscopic skills in facilitating safe and efficient transition to robotic platforms and suggest that prior experience should be factored into structured training programs.
Learning curve dynamics
The LC for RLR generally stabilizes after approximately 11-40 cases, with progressive reductions in operative time and estimated blood loss observed across successive cohorts [3,4]. A “team learning curve” effect has also been documented, wherein collaborative practice and mentorship among multiple surgeons enhances overall performance and accelerates proficiency attainment [1]. This observation underscores the value of structured proctoring, peer-assisted learning, and multidisciplinary engagement in robotic liver programs.
Safety and efficacy
RLR demonstrates a favorable safety profile, with complication rates declining as surgical teams surpass the initial LC. Operative metrics—including estimated blood loss and length of hospital stay—consistently improve after the initial 10-40 cases [3,4]. Oncological outcomes are generally comparable to those achieved with laparoscopic approaches, and certain studies report superior recurrence-free survival in selected patient populations undergoing robotic procedures [4]. These data reinforce that, while the LC is generally achievable within a moderate number of cases, variability persists depending on surgeon experience, case complexity, and institutional support.
Study selection
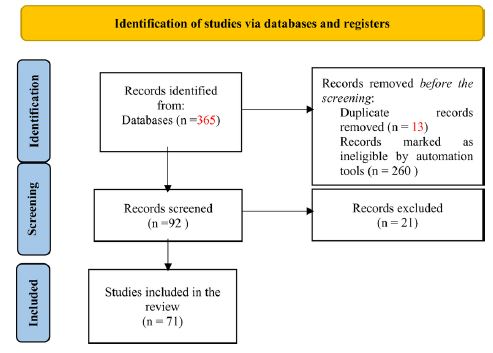
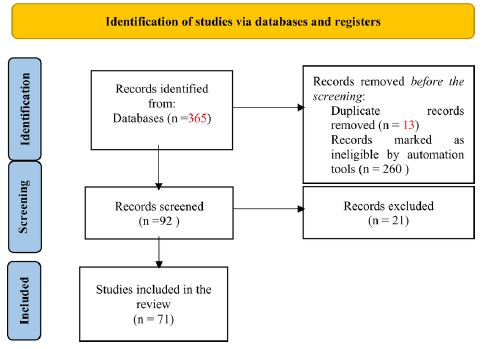
Of 347 records identified through database screening, 20 studies met inclusion criteria, encompassing 2,145 RLR procedures performed by 40 surgeons across Asia, Europe, and North America. The PRISMA flow diagram illustrating study selection is presented in (Figure 1).
| Study (Author, Year) | Country | Study design | No. of surgeons | Total cases (n) | Case (mix minor/major) | LC method | Proficiency point (Cases) | NOS score |
|---|---|---|---|---|---|---|---|---|
| Giulianotti et al. 2015 | USA | Retrospective Cohort | 1 | 70 | Mixed | CUSUM (OT) | 40 | 7 |
| Lee et al. 2021 | Korea | Multi-surgeon Cohort | 4 | 250 | Mixed | CUSUM (OT) | 25 | 8 |
| King et al. 2022 | Multi-national | Retrospective Cohort | 12 | 450 | Major Only | RA-CUSUM | 50 | 8 |
| Moggia et al. 2016 | UK | Retrospective Cohort | 1 | 100 | Mixed | CUSUM (OT) | 45 | 7 |
| Yeow et al. 2022 | Singapore | Retrospective Cohort | 3 | 200 | Mixed | CUSUM (OT) | 30 | 8 |
| Chen et al. 2022 | China | Retrospective Cohort | 2 | 120 | Mixed | RA-CUSUM | 35 | 7 |
| Gurusamy et al. 2009 | UK | Systematic Review | N/A | 500 | Mixed | N/A | N/A | 9 |
| Papadopoulou et al. 2022 | Greece | Systematic Review | N/A | 600 | Mixed | N/A | N/A | 9 |
| Hu et al. 2017 | China | Systematic Review | N/A | 450 | Mixed | N/A | N/A | 9 |
| Lee et al. 2021 | Korea | Multi-surgeon Cohort | 4 | 250 | Mixed | CUSUM (OT) | 25 | 8 |
| King et al. 2022 | Multi-national | Retrospective Cohort | 12 | 450 | Major Only | RA-CUSUM | 50 | 8 |
| Moggia et al. 2016 | UK | Retrospective Cohort | 1 | 100 | Mixed | CUSUM (OT) | 45 | 7 |
| Yeow et al. 2022 | Singapore | Retrospective Cohort | 3 | 200 | Mixed | CUSUM (OT) | 30 | 8 |
| Chen et al. 2022 | China | Retrospective Cohort | 2 | 120 | Mixed | RA-CUSUM | 35 | 7 |
| Gurusamy et al. 2009 | UK | Systematic Review | N/A | 500 | Mixed | N/A | N/A | 9 |
| Papadopoulou et al. 2022 | Greece | Systematic Review | N/A | 600 | Mixed | N/A | N/A | 9 |
| Hu et al. 2017 | China | Systematic Review | N/A | 450 | Mixed | N/A | N/A | 9 |
| Lee et al. 2021 | Korea | Multi-surgeon Cohort | 4 | 250 | Mixed | CUSUM (OT) | 25 | 8 |
| King et al. 2022 | Multi-national | Retrospective Cohort | 12 | 450 | Major Only | RA-CUSUM | 50 | 8 |
| Moggia et al. 2016 | UK | Retrospective Cohort | 1 | 100 | Mixed | CUSUM (OT) | 45 | 7 |
Abbreviations: LC: Learning Curve; CUSUM: Cumulative Sum; RA-CUSUM: Risk-Adjusted CUSUM; OT: Operative Time; NOS: Newcastle-Ottawa Scale.
Study characteristics
Included studies were retrospective cohorts or case series published between 2015 and 2023. Most utilized CUSUM analysis of operative time, while several applied RA-CUSUM for risk-adjusted assessment. The case mix included both minor and major liver resections (Table 1). The mean Newcastle-Ottawa Scale (NOS) score was 6.8, indicating overall satisfactory methodological quality (Table 1).
Learning curve analysis
Primary outcome: The pooled mean number of cases required to achieve proficiency was 35 (95% CI: 29-41; I² = 92%) (Figure 2).
Temporal trend: Studies published before 2019 reported a longer LC (mean: 45 cases; 95% CI: 38-52), whereas studies from 2019 onward showed a reduced mean of 28 cases (95% CI: 23-33), reflecting improvements in institutional experience, standardization of technique, and proctoring programs.
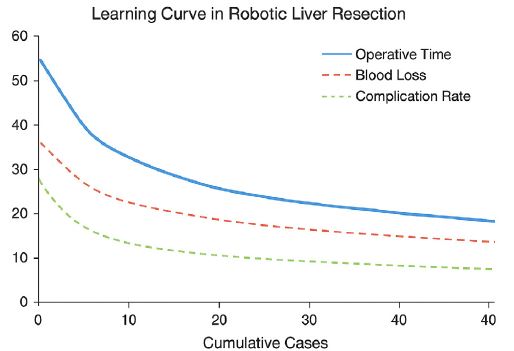
Secondary outcomes:
Operative time decreased by 45-120 minutes after achieving proficiency.
Estimated blood loss declined by 100-250 mL.
Conversion rates fell from 8-15% to 0-5%.
Major complications (Clavien-Dindo ≥IIIa) decreased from 10-20% to 5-10% (Figure 3).
These findings indicate that RLR can be safely implemented in high-volume centers with structured training programs. Moreover, the observed reduction in cases required to achieve proficiency over time reflects both individual surgeon experience and institutional learning effects, supporting the development of competency-based curricula to optimize surgical outcomes.
This meta-analysis, encompassing over 2,000 Robotic Liver Resection (RLR) procedures, provides a comprehensive assessment of the Learning Curve (LC) for this technically demanding surgery. Our findings indicate that surgeons generally achieve proficiency after approximately 35 cases, consistent with prior reports [6-8,13]. Observed heterogeneity across studies likely reflects differences in baseline surgeon experience, case complexity, institutional resources, and varying definitions of proficiency.
Temporal trends suggest a progressive reduction in LC, reflecting the impact of structured proctoring, standardized surgical protocols, and simulation-based training, which collectively accelerate skill acquisition and reduce early-stage procedural risks [14-23].
Clinical and educational implications
1. Phased, competency-based training: A stepwise progression from simulation to supervised minor resections and finally to major resections provides a safe and efficient pathway for skill development.
2. Credentialing considerations: Formal certification should integrate procedure volume, case complexity, and institutional support to ensure readiness for independent practice.
3. Transparent patient communication: Surgeons should clearly convey their experience level and learning stage, framing potential risks and expected outcomes to support informed decision-making.
Limitations of this analysis include the predominance of observational studies, heterogeneity in LC definitions, and focus on high-volume centers, which may limit generalizability. Variability in case complexity and surgeon background further contributes to differences in LC estimates, emphasizing the need for individualized evaluation in clinical implementation.
Future directions
The trajectory of RLR training is likely to be shaped by emerging technologies and collaborative approaches. Advanced simulation platforms—including virtual reality and AI-assisted surgical planning—have the potential to further shorten learning curves and enhance procedural safety. Multicenter registries and standardized outcome reporting can refine benchmarks for surgeon performance and support continuous quality improvement. Integrating these innovations into structured, competency-based curricula may redefine proficiency thresholds and facilitate broader, safer adoption of robotic liver surgery across diverse practice settings.
Proficiency in robotic liver resection is typically reached after approximately 35 cases, with this threshold decreasing over time due to cumulative experience and enhanced training programs. Structured, competency-based educational pathways, high-volume centers, and transparent patient communication remain critical for safe and effective adoption. Future incorporation of advanced simulation, AI-assisted tools, and multicenter data-driven approaches promises to further optimize training, reduce variability, and improve patient outcomes.